& EMERGENCY RESPONSE
This is the capstone of Course 8. Everything you've learned converges here — recognizing when a client is deteriorating, responding to system-specific emergencies, running a code, and evaluating whether your interventions are working.
RECOGNIZING CLINICAL DETERIORATION
Most cardiac arrests on hospital units are preceded by hours of warning signs that were missed or ignored. The nurse who recognizes deterioration early — and escalates — prevents the code from ever happening.
The Deterioration Ladder — from subtle to critical:
VS within normal limits, alert and oriented, adequate UOP, stable labs, pain controlled, wound healing as expected. Continue routine monitoring.
Subtle changes the nurse senses first: new restlessness or anxiety, "something's not right" feeling from client, mild tachycardia (HR 100–110), RR trending up (22–28), slight BP change, new confusion in elderly, decreased appetite, new complaint. Increase monitoring frequency. Assess further.
Clear deviation from baseline: HR >120 or <50, RR >28 or <8, SBP <90 or >200, SpO₂ <92% on O₂, new-onset confusion/agitation, UOP <0.5 mL/kg/hr × 2 hours, ↑ supplemental O₂ need, nurse worried despite "normal" VS. Call Rapid Response Team.
Unresponsive, pulseless, apneic, V-Fib/V-Tach/asystole/PEA on monitor, seizure activity, active hemorrhage with hemodynamic collapse, respiratory arrest. Call Code Blue. Begin BLS/ACLS immediately.
EARLY WARNING SCORING SYSTEMS & RAPID RESPONSE
▼Modified Early Warning Score (MEWS) / NEWS:
• Standardized scoring system using vital signs to identify deterioration
• Parameters scored: RR, HR, SBP, temperature, LOC, SpO₂, supplemental O₂ use
• Each parameter gets 0–3 points based on deviation from normal
• Higher score = higher risk of deterioration
• Score triggers actions: ↑ monitoring frequency, provider notification, rapid response activation
Rapid Response Team (RRT):
• Multidisciplinary team that responds to bedside emergencies BEFORE cardiac arrest
• Typically includes: ICU nurse, respiratory therapist, provider/NP/PA
• Any nurse can activate RRT — you don't need permission
• Common triggers:
→ VS outside parameters (per protocol)
→ Acute mental status change
→ Chest pain with new ECG changes
→ New-onset dyspnea/stridor
→ "I'm worried about this client" — clinical intuition is a valid trigger
SBAR communication for escalation:
• Situation: "I'm calling about Mr. Jones in 412. He's acutely deteriorating."
• Background: "He's post-op day 2 after colectomy. History of COPD, HF."
• Assessment: "HR has gone from 88 to 128 in the past hour. BP dropped from 124/72 to 86/50. RR 32. SpO₂ 88% on 4L NC. He's confused and diaphoretic."
• Recommendation: "I think he needs to be assessed immediately. I'd like to start a fluid bolus and get a stat CBC, lactate, and blood cultures."
CLINICAL INTUITION — "THE NURSE WHO JUST KNEW"
▼Why "gut feeling" matters in nursing:
• Research consistently shows that experienced nurses identify deterioration 6–8 hours before vital sign changes
• This isn't magic — it's pattern recognition from repeated exposure
• Subtle cues the brain processes: skin color shifts, breathing pattern changes, behavior changes, eye contact differences, voice tone changes
What to do when you "feel something is wrong" but VS are normal:
• Trust it — your clinical judgment is a valid assessment tool
• Increase monitoring frequency (VS q1h instead of q4h)
• Do a focused head-to-toe assessment — what specifically changed?
• Review trends: are any VS slowly trending in the wrong direction?
• Check labs if available
• Document your concerns specifically: "Client appears more lethargic than baseline. VS within parameters but trending: HR from 78 baseline to 98. Spoke with provider."
• NEVER downplay your instinct because the numbers look "okay"
The "failure to rescue" concept:
• Failure to rescue = recognizing a complication too late to prevent harm or death
• Most common cause: warning signs were present but not acted upon
• The NCLEX tests YOUR ability to be the nurse who escalates appropriately
• Better to call RRT and be wrong than to wait and be right about the code
The most dangerous phrase in nursing is "Let's just watch them." Watching is not an intervention. If you're worried enough to consider watching more closely, you're worried enough to assess more deeply, trend the data, and communicate your concern. The difference between "let's watch" and "I'm escalating" is sometimes the difference between a rapid response save and a code blue.
On the NCLEX, "notify the provider" is the right answer when assessment findings indicate deterioration beyond what nursing interventions can manage. But it's almost NEVER the FIRST action — assess first, intervene within your scope, THEN notify. The exception: findings that require immediate provider intervention (e.g., new STEMI, suspected stroke within thrombolytic window).
SEE IT COMING
Correct: B. The TRENDS tell the story — not any single measurement:
• HR trending up steadily (82→118) = compensatory tachycardia
• BP trending down steadily (132→96 systolic) = declining perfusion
• RR trending up (16→28) = respiratory compensation
• These together = classic early compensatory shock pattern
• The client saying "something isn't right" adds clinical weight
Individual values might still look "within normal limits" (A, D), but the direction is unmistakable. Pain (C) wouldn't cause progressive BP decline. SpO₂ of 96% is a lagging indicator — it drops LATE in shock. By the time SpO₂ drops, the client may be coding. Trends trump individual values.
Correct: C. SBAR components:
• Situation (B) — why you're calling: "his condition has changed"
• Background (A) — relevant history: post-op, comorbidities
• Assessment (C) — YOUR clinical findings AND interpretation: VS changes + physical findings + what you think is happening ("I believe he may have developed a PE")
• Recommendation (D) — what you think should be done: specific orders requested
The Assessment is where the nurse demonstrates clinical judgment — not just reporting numbers, but synthesizing them into a clinical picture. This is the most powerful part of SBAR because it tells the provider what the nurse is seeing at the bedside.
Correct: B. Clinical intuition deserves investigation, not dismissal:
• VS are currently normal — RRT (A) is premature without any objective finding
• But dismissing the concern entirely (C) ignores the evidence that nurse intuition frequently precedes measurable deterioration
• The right response: dig deeper
→ Focused reassessment (what specifically seems different?)
→ Increase monitoring frequency
→ Review trend data for any subtle shifts
→ Document the concern
• Medicating the client (D) doesn't address the nurse's clinical observation and is inappropriate
• If the deeper assessment reveals concerning trends → THEN escalate
SYSTEM-SPECIFIC EMERGENCIES
Each body system has its own catastrophic failure mode. The NCLEX tests whether you can identify the emergency, prioritize the interventions, and act without hesitation.
Tap each card to review the emergency response:
PULMONARY EMBOLISM
Tap for emergency response
• D-dimer: if elevated → CT angiogram to confirm
• ABG: respiratory alkalosis (hyperventilation) initially
• Treatment: anticoagulation (heparin → warfarin/DOAC), thrombolytics if massive PE with hemodynamic instability
• Prevention: SCDs, early ambulation, LMWH prophylaxis
ACUTE STROKE
Tap for emergency response
• Hemorrhagic (13%): vessel rupture → tPA CONTRAINDICATED
• Assessment: FAST (Face/Arms/Speech/Time), NIH Stroke Scale
• CT scan FIRST (rule out hemorrhage before tPA)
• BP: permissive hypertension (maintain perfusion) unless >220/120 or tPA planned
• tPA eligibility: onset <4.5 hr, no bleeding, no recent surgery
ANAPHYLAXIS
Tap for emergency response
• EPINEPHRINE IM (anterolateral thigh) = FIRST and ONLY life-saving drug
• Adult dose: 0.3–0.5 mg of 1:1000 IM, repeat q5–15 min
• Then: IV fluids, antihistamines (diphenhydramine), steroids, nebulized albuterol for bronchospasm
• Observe 4–6 hours (biphasic reaction risk)
• Epinephrine FIRST — everything else is supportive
ACUTE MI — STEMI RESPONSE
▼Recognition:
• Chest pain: crushing, substernal, radiating to jaw/left arm/back
• Diaphoresis, dyspnea, nausea
• Atypical presentation (common in women, elderly, diabetics): fatigue, indigestion, back pain, no chest pain
• ECG: ST elevation in 2+ contiguous leads = STEMI
MONA + more (initial management):
• Morphine (if pain unresponsive to nitroglycerin — use cautiously, not routine)
• Oxygen (only if SpO₂ <94% — routine O₂ not indicated in uncomplicated MI)
• Nitroglycerin SL × 3 (q5 min — contraindicated if SBP <90 or if PDE5 inhibitor used within 24–48 hours)
• Aspirin 162–325 mg chewed (antiplatelet — reduces mortality)
• Heparin IV, clopidogrel or ticagrelor (dual antiplatelet therapy)
• STEMI: PCI (percutaneous coronary intervention) within 90 minutes = goal — door-to-balloon time
• If PCI not available within 120 min → fibrinolytics
Post-MI nursing priorities:
• Continuous cardiac monitoring
• Serial troponins (q3–6h × 3 — trending confirms MI)
• Bedrest initially → progressive activity
• Monitor for complications: arrhythmias (#1), heart failure, cardiogenic shock, papillary muscle rupture, ventricular wall rupture, pericarditis (day 2–3)
• Discharge meds: "ABCDE" — ACE inhibitor, Beta-blocker, Cholesterol (statin), Dual antiplatelet, Exercise/Education
HEMORRHAGIC EMERGENCIES — MASSIVE TRANSFUSION
▼Massive hemorrhage indicators:
• Loss of one entire blood volume in 24 hours (~5 L in adult)
• Need for ≥10 units PRBCs in 24 hours
• Active bleeding with hemodynamic instability unresponsive to crystalloids
Massive Transfusion Protocol (MTP) activation:
• Coordinated release of blood products in fixed ratios
• Goal: 1:1:1 ratio of PRBCs : FFP : platelets (damage control resuscitation)
• Prevents dilutional coagulopathy from giving PRBCs alone
• Warmed blood products (prevent hypothermia → coagulopathy worsens)
• Monitor for: hypocalcemia (citrate in stored blood binds Ca²⁺), hyperkalemia (stored blood releases K⁺), hypothermia
Transfusion reactions — recognize immediately:
• Acute hemolytic: ABO incompatibility → fever, chills, flank pain, hemoglobinuria (dark urine), hypotension → STOP transfusion immediately, NS via new line, notify provider, send blood/urine to lab
• Febrile non-hemolytic: most common reaction → fever, chills without hemolysis → stop transfusion, antipyretics, rule out hemolytic first
• Allergic: urticaria, itching → stop transfusion, antihistamine. If anaphylactic → epinephrine
• TRALI (Transfusion-Related Acute Lung Injury): acute dyspnea, bilateral infiltrates, hypoxemia within 6 hours → supportive care (similar to ARDS)
• TACO (Transfusion-Associated Circulatory Overload): dyspnea, hypertension, JVD, crackles → diuretics, slow or stop transfusion
Nursing priority for ALL reactions: STOP the transfusion, maintain IV access with NS, notify provider, send blood bag + tubing + client blood/urine samples to lab
METABOLIC EMERGENCIES — HYPERKALEMIA & HYPOGLYCEMIA
▼Hyperkalemia emergency (K⁺ >6.5):
• ECG: peaked T waves → widened QRS → sine wave → V-fib/asystole
• Treatment sequence:
1. Calcium gluconate IV — stabilizes cardiac membrane (doesn't lower K⁺)
2. Insulin + D50 — drives K⁺ into cells (temporary)
3. Sodium bicarbonate — shifts K⁺ into cells
4. Albuterol nebulizer — shifts K⁺ into cells
5. Kayexalate — binds K⁺ for GI excretion
6. Dialysis — definitive removal
Severe hypoglycemia (glucose <40 mg/dL):
• Signs: tremor, diaphoresis, confusion, seizures, LOC, coma
• Conscious client: 15 g fast-acting carbohydrate → recheck in 15 min → repeat if still low (Rule of 15)
• Unconscious client: D50 IV push (25 g dextrose) or glucagon IM/SubQ if no IV access
• NEVER give oral glucose to an unconscious client (aspiration risk)
• After correction: follow with protein and complex carb snack to prevent rebound hypoglycemia
• Investigate cause: missed meal, too much insulin, medication error, renal failure (insulin not cleared)
Transfusion reaction: STOP first, then work the problem. For ANY suspected transfusion reaction — stop the transfusion immediately. Keep the IV open with NS through a NEW line (don't flush the blood line). Save the blood bag and tubing. Then assess, intervene based on the type of reaction, and notify the provider. The blood bank needs the bag back.
In anaphylaxis, epinephrine is not optional — it IS the treatment. Antihistamines treat hives. Steroids prevent recurrence. Bronchodilators open airways. But ONLY epinephrine reverses the cardiovascular collapse and upper airway obstruction that kills. If the NCLEX gives you anaphylaxis, epinephrine is always the first drug — everything else is second.
RESPOND TO THE CRISIS
Correct: A. The triad of fever + flank/back pain + hemoglobinuria (dark urine) + hypotension = classic acute hemolytic transfusion reaction from ABO incompatibility.
• Donor RBCs are destroyed → hemoglobin released → hemoglobinuria (dark urine)
• Flank pain from renal damage as hemoglobin precipitates in kidneys
• Hypotension from massive inflammatory cascade
Actions: STOP transfusion immediately → NS via new line → notify provider + blood bank → send blood bag + tubing + client blood and urine samples to lab → fluid resuscitation → monitor for DIC and renal failure.
Febrile non-hemolytic (B) doesn't cause dark urine or back pain. TRALI (C) presents with respiratory distress, not hemoglobinuria. Allergic (D) presents with urticaria, not back pain.
Correct: A. This is a tPA-eligible ischemic stroke:
• Symptom onset: 2 hours ago (within 4.5-hour window)
• CT: no hemorrhage (hemorrhagic stroke ruled out)
• Classic stroke symptoms: unilateral weakness, facial droop, dysarthria
tPA (alteplase) is the definitive treatment — dissolves the clot and restores blood flow. Time is brain — every minute of delay = ~1.9 million neurons lost.
Heparin (B) is NOT used acutely in ischemic stroke (doesn't dissolve existing clot). Aggressive BP lowering (C) is contraindicated — permissive hypertension maintains cerebral perfusion. MRI (D) delays treatment — CT is sufficient to rule out hemorrhage and guide tPA decision.
Correct: C. This is anaphylaxis — urticaria + angioedema + stridor + hypotension = multi-system allergic emergency.
EPINEPHRINE IM is ALWAYS first. It is the ONLY drug that:
• Reverses bronchospasm (beta-2 effect)
• Reduces angioedema and urticaria (alpha-1 vasoconstriction → decreases vascular permeability)
• Increases BP (alpha-1 vasoconstriction + beta-1 cardiac stimulation)
• Inhibits further mast cell degranulation
Diphenhydramine (A) treats hives but cannot reverse airway obstruction or shock. Steroids (B) prevent biphasic reaction but take hours to work. Albuterol (D) helps wheezing but won't address the stridor (upper airway) or cardiovascular collapse. No other drug saves the anaphylaxis patient — only epinephrine.
CODE MANAGEMENT & EVALUATING EMERGENCY INTERVENTIONS
When the code is called, organized chaos must become organized response. Every team member has a role. The NCLEX tests whether you understand the algorithm, can prioritize in real-time, and can evaluate whether the interventions are actually working.
- 1RECOGNIZE → CHECK PULSE → CALL CODE → START CPR
• Unresponsive + no breathing/agonal gasps + no pulse within 10 seconds
• Call for help / activate Code Blue
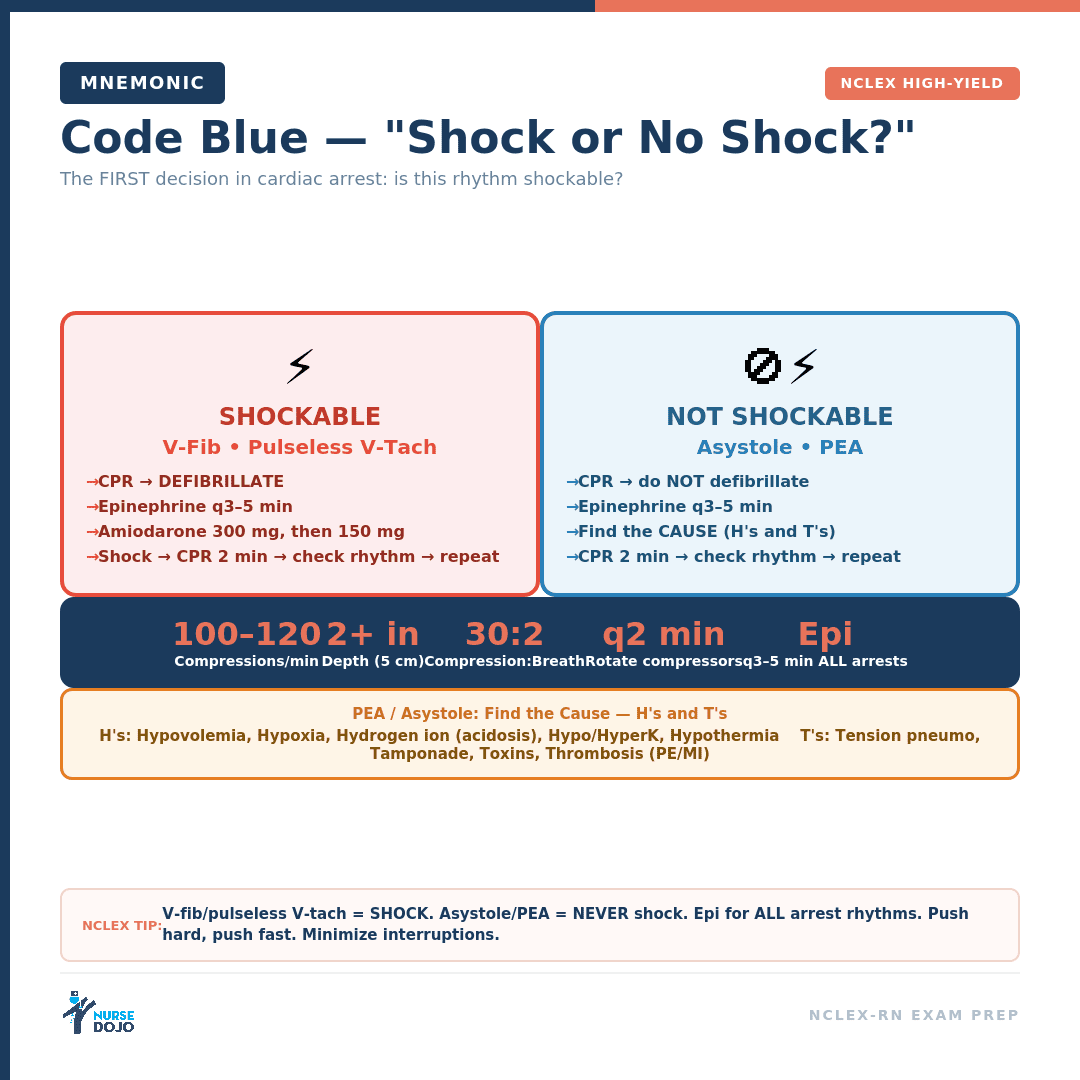
• Begin high-quality CPR immediately: rate 100–120/min, depth 2–2.4 inches, full recoil, minimize interruptions - 2IDENTIFY THE RHYTHM → SHOCKABLE OR NOT?
• Shockable: V-Fib or pulseless V-Tach → DEFIBRILLATE (unsynchronized)
• Non-shockable: Asystole or PEA → CPR + epinephrine (no shock) - 3SHOCKABLE PATHWAY (V-Fib / Pulseless V-Tach):
• Shock → immediately resume CPR × 2 minutes → rhythm check
• Epinephrine 1 mg IV/IO q3–5 min (after 2nd shock)
• Amiodarone 300 mg IV (after 3rd shock), then 150 mg
• Continue cycle: CPR → rhythm check → shock if still shockable → drugs - 4NON-SHOCKABLE PATHWAY (Asystole / PEA):
• CPR → epinephrine 1 mg IV/IO q3–5 min → CPR × 2 min → rhythm check
• Search for and treat REVERSIBLE causes (H's and T's)
• No shock, no amiodarone (nothing to shock in asystole, organized but pulseless in PEA)
Reversible Causes — H's
• Hypovolemia — volume replacement (fluids, blood)
• Hypoxia — oxygenation, advanced airway
• Hydrogen ion (Acidosis) — sodium bicarbonate, ventilation
• Hypo/Hyperkalemia — calcium gluconate (hyper), potassium replacement (hypo)
• Hypothermia — rewarming ("warm and dead" rule)
• Hypoglycemia — D50 IV push
Reversible Causes — T's
• Tension pneumothorax — needle decompression (2nd ICS, midclavicular)
• Tamponade (cardiac) — pericardiocentesis
• Toxins/Tablets — specific antidotes (naloxone, flumazenil, digoxin immune fab, etc.)
• Thrombosis (coronary) — PCI or fibrinolytics
• Thrombosis (pulmonary / PE) — thrombolytics, surgical embolectomy
HIGH-QUALITY CPR — THE NON-NEGOTIABLES
▼Compression quality makes or breaks the code:
• Rate: 100–120 compressions per minute (not faster — loses effectiveness)
• Depth: at least 2 inches, no more than 2.4 inches (adults)
• Full chest recoil between compressions (don't lean on the chest)
• Minimize interruptions (<10 seconds for rhythm checks, <10 seconds for shock)
• Rotate compressors every 2 minutes (fatigue degrades quality rapidly)
• Compression-to-ventilation ratio: 30:2 without advanced airway, continuous with advanced airway
• Hard, flat surface (use backboard if in bed)
Advanced airway during CPR:
• Once ETT or supraglottic airway placed → continuous compressions (no pauses)
• Ventilate: 1 breath every 6 seconds (10 breaths/min)
• Avoid hyperventilation → ↑ intrathoracic pressure → ↓ venous return → worse outcomes
• Confirm placement with waveform capnography (ETCO₂)
ETCO₂ during CPR — the quality monitor:
• ETCO₂ >10 mmHg during CPR = adequate compressions generating cardiac output
• ETCO₂ <10 mmHg = poor compressions → improve technique
• Sudden ↑ in ETCO₂ (>40) = possible ROSC → check pulse
• ETCO₂ is the best real-time indicator of CPR quality and ROSC
EVALUATING EMERGENCY INTERVENTIONS — IS IT WORKING?
▼During a code — signs of ROSC (Return of Spontaneous Circulation):
• Sudden sustained ↑ in ETCO₂ (typically >40 mmHg)
• Palpable pulse with rhythm check
• Arterial waveform on A-line (if present)
• Spontaneous breathing, movement, or eye opening
• ↑ BP on monitoring
Post-ROSC care priorities:
• 12-lead ECG → if STEMI → emergent PCI
• Targeted temperature management (32–36°C × 24 hours)
• Hemodynamic optimization: MAP >65, adequate oxygenation (SpO₂ 92–98%), avoid hyperoxia
• Avoid hyperventilation (can ↓ cerebral blood flow)
• Continuous monitoring: ECG, VS, neuro status, labs (lactate, ABG, electrolytes)
• Seizure monitoring and treatment
Evaluating effectiveness OUTSIDE of codes:
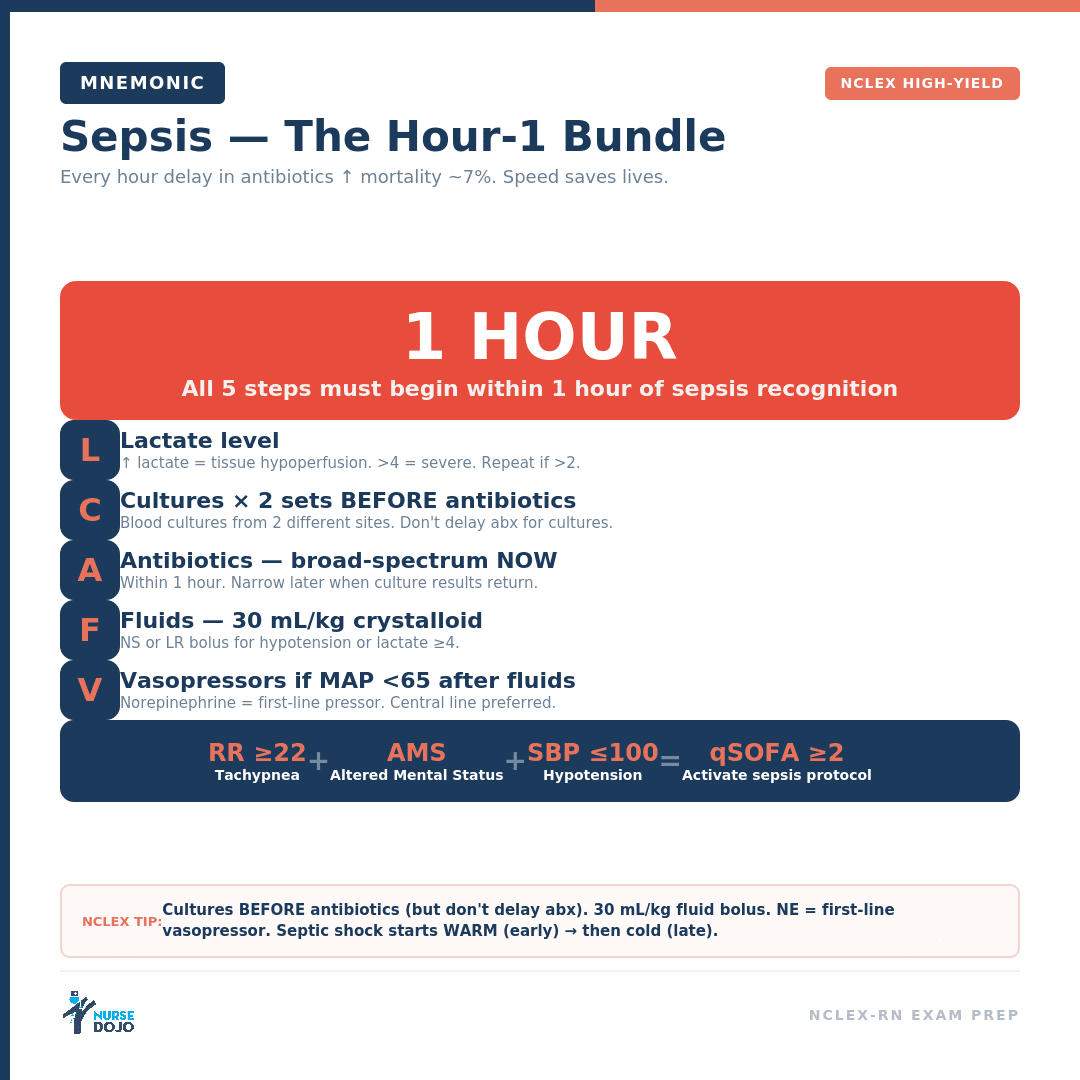
• Sepsis treatment: lactate trending DOWN (best indicator), MAP >65, UOP improving, mental status clearing
• Heart failure treatment: ↓ crackles, ↓ dyspnea, ↓ weight (diuresis), ↑ UOP, ↓ BNP
• Hemorrhage treatment: HR trending down, BP stabilizing, ↑ UOP, H&H stabilizing on serial draws
• Respiratory failure treatment: SpO₂ improving, RR normalizing, ABGs improving, ↓ work of breathing
• General principle: improving END-ORGAN perfusion (brain=LOC, kidneys=UOP, skin=color/temp) is the real measure — not just the numbers on the monitor
A nurse finds a client unresponsive in bed. No pulse is palpable. The monitor shows a chaotic, irregular waveform with no identifiable complexes. The code team is arriving.
Within the first 30 seconds:
• Confirm unresponsive + pulseless (check carotid ≤10 seconds)
• Call Code Blue (if not already activated)
• Begin CPR — chest compressions immediately (hard and fast, 100–120/min, 2+ inches deep)
• Place backboard under client
• Rhythm: chaotic + no identifiable complexes = Ventricular Fibrillation
• This is a SHOCKABLE rhythm → prepare the defibrillator
Shock + CPR cycle:
• Charge defibrillator while CPR continues
• Clear → DEFIBRILLATE (unsynchronized, biphasic 120–200 J)
• Immediately resume CPR for 2 minutes (do NOT stop to check rhythm after shock)
• Establish IV/IO access during CPR
• Prepare epinephrine and amiodarone
• Place advanced airway when feasible (don't interrupt compressions)
• Assign roles: compressor, airway, IV/meds, recorder, timer
• Rotate compressors at the 2-minute mark
2-minute rhythm check → still V-Fib:
• Shock #2 → resume CPR
• Epinephrine 1 mg IV push → flush → continue CPR
• 2-minute check → still V-Fib:
• Shock #3 → resume CPR
• Amiodarone 300 mg IV push
• Continue cycle: CPR → check → shock → epi q3–5 min → amiodarone 150 mg (2nd dose)
• Search for reversible causes (H's and T's)
• Monitor ETCO₂ — >10 = good compressions, sudden ↑ >40 = possible ROSC → check pulse
If rhythm changes to asystole/PEA:
• Switch to non-shockable pathway: CPR + epinephrine only (no shock, no amiodarone)
• Aggressively search for and treat reversible causes
When ROSC achieved:
• Confirm: pulse present, BP measurable, ETCO₂ >40 sustained
• Post-ROSC: 12-lead ECG, TTM, ICU, hemodynamic optimization, neuro monitoring
The defibrillator doesn't save the patient. CPR saves the patient. Defibrillation resets the electrical system. But without CPR maintaining coronary and cerebral perfusion between shocks, there's nothing left to reset. High-quality compressions — hard, fast, full recoil, minimal interruptions — are the single most important intervention in any cardiac arrest. Everything else is built on top of CPR.
PUT IT ALL TOGETHER
Correct: A. ETCO₂ during CPR is the real-time quality indicator:
• >10 mmHg = adequate compressions generating cardiac output
• <10 mmHg = compressions are NOT effective — blood is not circulating enough to carry CO₂ to the lungs
• Sudden rise >40 mmHg = possible ROSC
ETCO₂ of 8 × 4 minutes = the team needs to improve CPR quality: deeper compressions, correct rate, ensure full recoil, rotate to a fresh compressor. ETCO₂ is NOT "expected to be low" (B) — it reflects CPR effectiveness. It's very reliable during CPR (D) and is recommended by AHA guidelines. ETT misplacement (C) is possible but would show very low or absent ETCO₂ from the start, not a sustained 8.
Correct: B. Asystole = non-shockable rhythm. There is NO electrical activity to reset — defibrillation (A) is useless and harmful (delays CPR). The algorithm:
• High-quality CPR (the foundation)
• Epinephrine 1 mg IV/IO q3–5 min (stimulates cardiac activity)
• Search for and treat reversible causes (H's and T's) — this is where the real chance of saving the patient lies
Amiodarone (C) is for V-Fib/V-Tach only — it's an antiarrhythmic for shockable rhythms. Transcutaneous pacing (D) is for symptomatic bradycardia with a pulse, not asystole. In asystole, the myocardium often has no viable electrical or mechanical activity to pace.
Correct: B. Post-ROSC with STEMI (ST elevation in II, III, aVF = inferior MI):
• The MI likely CAUSED the cardiac arrest
• Emergent PCI = #1 priority to open the occluded coronary artery
• Without revascularization → re-arrest is highly likely
• Door-to-balloon target applies even in post-arrest patients
FiO₂ 100% (A) should actually be weaned — SpO₂ 100% = hyperoxia post-ROSC → generates free radicals → worsens neurological outcome. Target SpO₂ 92–98%. TTM (C) is important but doesn't take priority over fixing the cause of the arrest. Amiodarone (D) is supportive but revascularization is the definitive treatment.
Correct: B. The best indicators of effective sepsis treatment are end-organ perfusion markers:
• Lactate clearing (6.2 → 2.8) = tissues getting oxygen again (best single indicator)
• MAP >65 (56 → 72) = perfusion pressure restored
• UOP improving (10 → 48 mL/hr) = kidneys being perfused
• Mental status improving = brain being perfused
Temperature and WBC (A) may take days to normalize — they're infection markers, not perfusion markers. Vasopressor weaning (C) is a positive sign but doesn't confirm organ perfusion as directly. CVP alone (D) tells you about volume status but not whether that volume is reaching the organs. Lactate + UOP + LOC = the sepsis treatment scorecard.
TRAINING COMPLETE!
You've completed Module 8.8 — the final module of Course 8: Physiological Adaptation. You now have the clinical judgment to recognize deterioration, respond to emergencies, run a code, and evaluate whether your interventions are saving the patient.
EMERGENCY MASTERY — COURSE 8 CAPSTONE
- 1Deterioration recognition: Trends trump individual values. HR↑ + BP↓ + RR↑ = compensatory shock pattern. Nurse intuition is valid — investigate further when "something feels off." Use SBAR to escalate. Activate RRT before the code happens.
- 2PE: Sudden dyspnea + pleuritic chest pain + tachycardia + hypoxemia. D-dimer → CT angio. Treatment: anticoagulation, thrombolytics if massive. Prevention: SCDs + LMWH + early ambulation.
- 3Stroke: FAST assessment. CT FIRST to rule out hemorrhage. tPA within 4.5 hours for ischemic stroke. Permissive hypertension. Time is brain — every minute = neurons lost.
- 4Anaphylaxis: Epinephrine IM = FIRST and ONLY life-saving drug. 0.3–0.5 mg IM anterolateral thigh. Then: fluids, antihistamines, steroids, bronchodilators. Observe for biphasic reaction.
- 5MI (STEMI): Aspirin chewed + NTG SL + heparin + PCI within 90 min. Post-MI: ABCDE discharge meds. Watch for arrhythmias (#1 complication), HF, cardiogenic shock.
- 6Transfusion reactions: STOP the blood first. Hemolytic = fever + back pain + dark urine. Save the bag. NS via new line. For ALL reactions: stop → NS → notify → send specimens.
- 7ACLS algorithm: Shockable (V-Fib/pV-Tach) → defibrillate + CPR + epi + amiodarone. Non-shockable (asystole/PEA) → CPR + epi only + find reversible cause (H's and T's). ETCO₂ >10 = good CPR. Sudden ETCO₂ >40 = ROSC.
- 8Evaluating effectiveness: Sepsis → lactate clearing + UOP + mental status. HF → ↓crackles + ↓weight + ↑UOP. Hemorrhage → ↓HR + ↑BP + stabilizing H&H. Post-ROSC → STEMI check → PCI, TTM, avoid hyperoxia (SpO₂ 92–98%).
This entire course has been about one thing: the nurse who sees what's coming. The nurse who notices the trend before it becomes a crisis. The nurse who trusts their instinct and escalates. The nurse who runs toward the code, not away from it. The nurse who knows the algorithm, delivers perfect compressions, and evaluates whether the treatment is actually working — not just whether it was given. Physiological Adaptation isn't a topic. It's the reason nursing exists. The body fails. The nurse adapts. The patient survives.
Cheat Sheet
Black belt recall